
Groundbreaking Study, and Solutions for long COVID Patients
This study from UCSF is important


After many years of suffering, long COVID patients have more answers. A groundbreaking UCSF study reveals why symptoms persist - and more importantly, what you can do about it.
Yesterday I uploaded a video on YouTube reviewing a study from the University of California San Francisco (UCSF). This study provides evidence for persistent SARS-COV-2 virus even after 2 years, and a resultant activated immune system continuing to cause inflammation.
(Side note: I have listed my best inflammation and solutions videos at the end of this article.)
Here is the video for your viewing pleasure: https://youtube.com/live/BaUl3JtGaks
Long COVID: Why Won’t It Stop? (New Study Reveals the Answer) - YouTube
What Did They Find?
The researchers found two main things: viral persistence and T cell activation. Let me break these down.
Viral Persistence
Even after 2+ years, they found double stranded RNA (dsRNA) of the spike protein in body tissues of long COVID patients. Now, dsRNA is important because it’s a replication intermediate - it only shows up when a virus is actively replicating inside our cells.
Here’s the key point: this dsRNA cannot come from the vaccine. The vaccine mRNA is already in its final form. But when the actual virus replicates, it has to go through multiple steps, and one of those steps is making dsRNA. So this is evidence of ongoing viral replication.
T Cell Activation Throughout the Body
The researchers also found that T cells are activated in the tissues - specifically in spinal cord, gut (GIT), and lung tissues. And here’s what’s interesting: the patients who had activated T cells in these specific locations had corresponding symptoms. Spinal cord activation correlated with neurological symptoms, GIT activation with digestive issues, and so on.
These activated T cells release cytokines that cause inflammation - not just locally, but throughout the body. And here we go for the long COVID symptoms.
So now we understand the mechanism. Let’s talk about what we can do about it before we dive a bit more deeper into the science.
How do we solve it?
Disclaimer: following is not a medical advice. Discuss with your doctor and figure out the best approach for yourself.
Lifestyle Changes
Intermittent fasting
Near infrared light
Red light
Forest bathing and other means to reduce stress
Sleep
Light exercise
Etc.
Diet
Low histamine diets
No left-over food (develops histamine and other inflammatory toxins)
Mediterranean diet
Low carbs/low sugars (sugars boost the activity of already active immune system.)
Omega 3
Antioxidants both that work in water and in lipids i.e. Vitamin C and Vitamin E
Immune modulators (Vitamin D, Curcumin, NAC etc.)
Blood vessel health (L-arginine, nattokinase, etc.)
Fruits
Vegetables
Green tea
Fruits and vegetables with red color in them (quercetin) with zinc
Pomegranate (contains Urolithin A)
Etc.
Allopathic medicines
Disease modifying antirheumatic drugs (DMARDs) like abatacept, TNF inhibitors, etc.
Low dose naltrexone
Ivermectin
Short burst of steroid therapy (Medrol pack)
Etc.
None of the categories above are exhaustive, but good start.
Now the science.
Virus Persists in Tissue Reservoirs in Some Patients
The takeaway is that the researchers found double stranded RNA (dsRNA) of the spike protein in some body tissues of the long COVID patients. dsRNA is a viral replication intermediate. That is, it is made in our cells when a virus is actively replicating. All except one participants were vaccinated, however, this dsRNA cannot come from a vaccine as the vaccine mRNA is already in the final workable state. However, the virus RNA manufacturing needs to go through multiple steps including dsRNA formation.
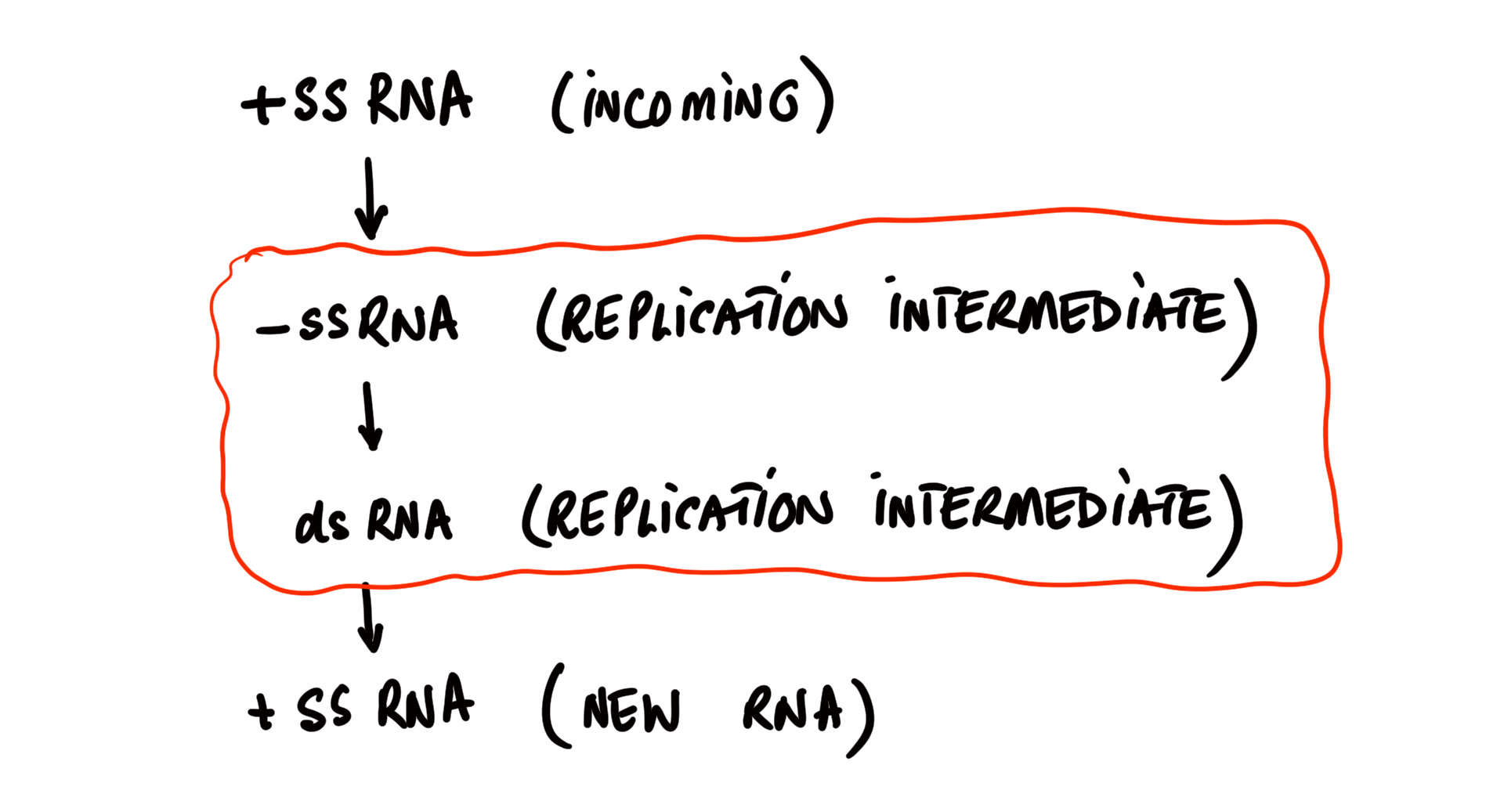
Figure 1: SARS-COV-2 enters our cells having positive sense single stranded RNA (+ssRNA). Part of the replication process is to make negative single stranded RNA (-ssRNA). Positive and negative sense RNA combine to make double stranded RNA (dsRNA). And, finally +ssRNA are made that will be contributed to the newly formed viruses.
Why Does the Virus Persist?
Researchers’ conjecture is that it may be due to the failure of our immune system to clear the virus from some tissues, or local replication with limited viral spread. But, basically by an unknown mechanism.
Researchers write:
Double-stranded SARS-CoV-2 RNA was also identified in gut lamina propria in three of the four participants with detectable single-stranded RNA (ssRNA) in all three gut regions surveyed (Table 1). Double-stranded RNA (dsRNA) is only produced during active viral transcription and translation activity or during replication. We observed intracellular dsRNA in relatively discrete clusters and not distributed widely across all regions, which may represent either local replication with limited viral spread or lack of ability to achieve immune clearance of actively infected cells
Tissue Based T Cells are Found Activated
Next the researchers found that the T Cells are activated throughout the body. However, individuals who had activated T cells in their spinal cord, GIT, or pulmonary tissues had long COVID symptoms most common of which was fatigue, the most common symptom set was for neurological symptoms, then GIT, and then other tissues.
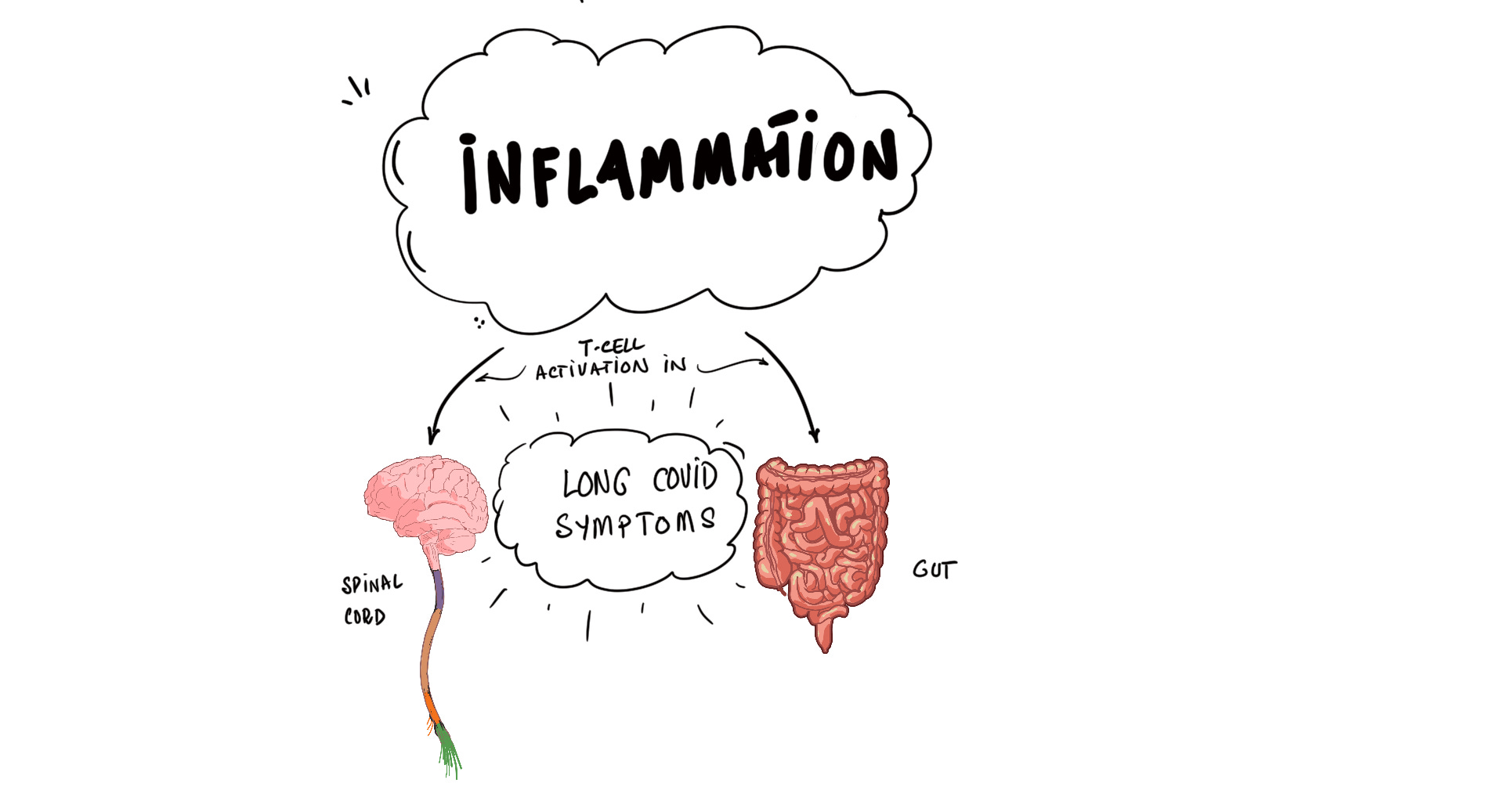
Figure 2: researchers found evidence of replicating virus and resultant immune activation leading to inflammation. Long COVID symptoms were present in individuals with immune activation in spinal cord or GIT.
The researchers also found CD68+ cells (macrophages) activated in the tissues where viral dsRNA was observed. These are macrophages. The role of a macrophage is to break down foreign offending agents or virally infected cells and present parts of the offending agent to T cells.
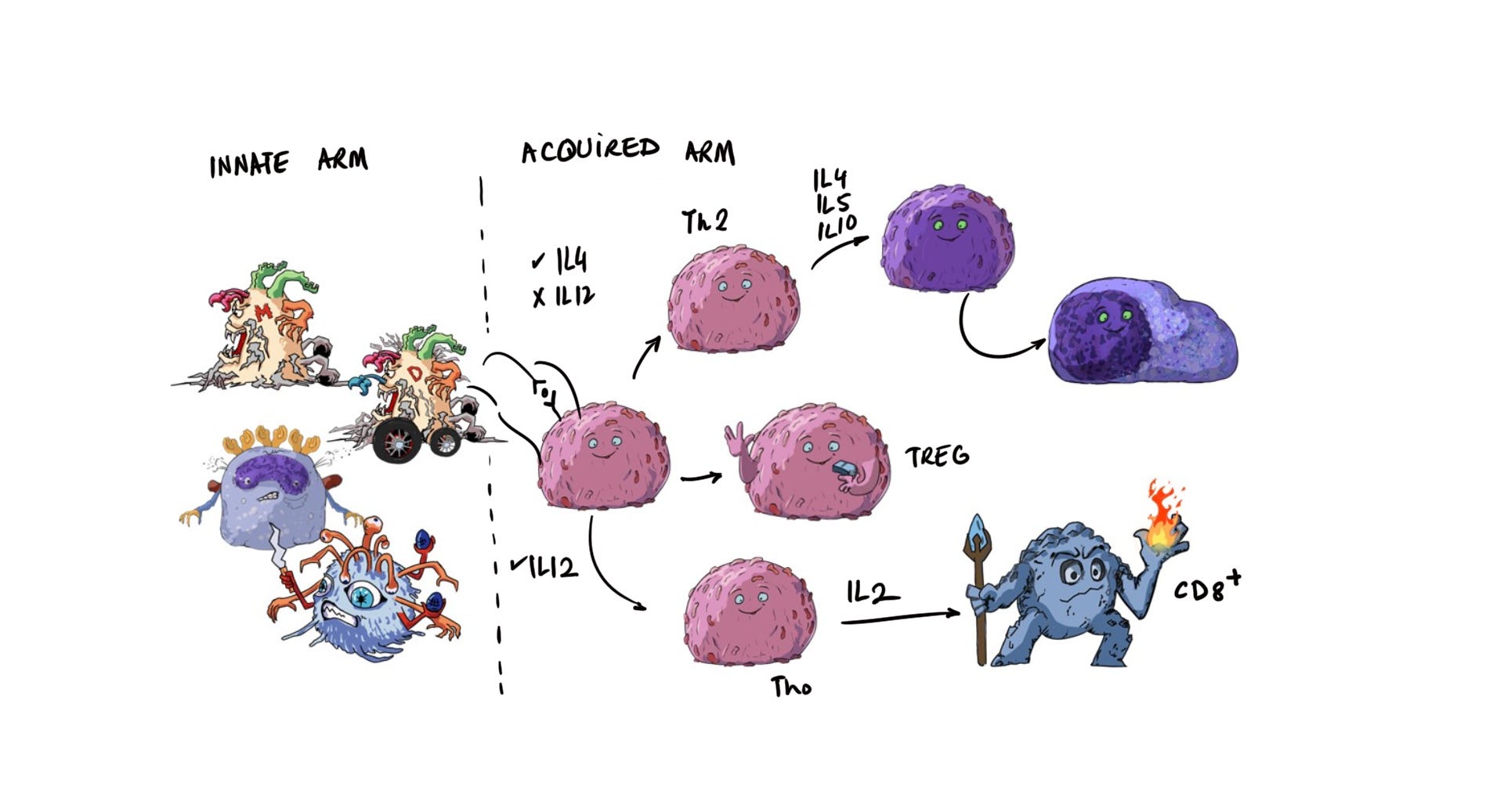
Figure 3: a virus or a virally infected cell will activate the innate arm cells (CD68+ cells found in this study), which in turn will activate the T cells on the acquired arm side. These T cells in turn can lead to activation of cytotoxic cells (CD8+) and/or B cells to make antibodies (dark purple cells on the upper right).
These cells will also release cytokines to cause inflammation not in the local tissue but throughout the body. And, here we go for the long COVID symptoms.
I will recommend you look at the study or watch my video for a further detailed analysis and review.
Also, I have recorded a number of videos about inflammation. It will be helpful for you to inform yourself of these mechanics and their modulators. Wishing you health!
My discussions for inflammatory pathways (paid access - supports my work.)
How does spike protein cause inflammation? - YouTube
OTC Inflammation Treatments: What Works and What’s Hype? - YouTube
Stop Inflammation, Protect Your Brain - YouTube
Fixing Chronic Inflammation - Why Did You Not Get Inflamed When Younger? - YouTube
Inflammation in The Body Damages Brain Tissue - YouTube
How to Reduce Glycation? (A Huge Contributor to Aging and Chronic Inflammation.) - YouTube
Beat Chronic Inflammation with This 3-Step Plan - YouTube
Long COVID: Why Won’t It Stop? (New Study Reveals the Answer) - YouTube
Got Inflammation? Discover Urolithin A - YouTube
The study reviewed: Tissue-based T cell activation and viral RNA persist for up to 2 years after SARS-CoV-2 infection
Visit drbeen.com for more lectures.
This paper is a year old and I am not an expert on anything, but I feel this article introduces something worth looking at in terms of understanding COVID damages that can't be linked to spike protein.
The Long-COVID Syndrome: Neoantigens as Driving Force for the Onset of Autoimmune Diseases - Rolf Marschalek
Rolf Marschalek has come up in the rececent McKernan et. al. oncology publication controversy.
Marschalek proposes eternal vaccination for COVID, and has his biases. But I feel that his theoretical paper below discusses a potentially worthy piece of the puzzle. Adding a massive number bad things to the virus does not detract from the massive number of bad things about the mRNA vaccines. Both are on the same side of the teeter-totter.
He seems to be trying to cast attention away from engineered Spike, but it was the first time I had read of the 2 nasty proteases in Covid-19 (and shared by MERS and other viruses).
It sounds like a nasty process, not unique to our favorite bat flu - and if it's going on in addition to the multifaceted spike injuries, it adds even more static to the signals. We can talk about autoimmunity from overproduced spike motifs and numerous frameshift off-targets, and contaminated shots, but he is talking about self proteins directly being added to the autoimmune attack from viral NSP5(3CLPro) and NSP3(PLPro).
---
Copilot:
The Long-COVID Syndrome: Neoantigens as Driving Force for the Onset of Autoimmune Diseases - Rolf Marschalek
Summary of the Paper
The title "The Long-COVID Syndrome: Neoantigens as Driving Force for the Onset of Autoimmune Diseases" refers to a 2025 commentary article (often classified as an open-access commentary or hypothesis paper) authored by Rolf Marschalek, published in the Journal of Cellular Immunology (Volume 7, Issue 1, pages 26–31). scientificarchives.com
Central Hypothesis
Marschalek proposes that Long COVID (LC, also known as post-acute sequelae of SARS-CoV-2 infection) is primarily an autoimmune disorder triggered by the massive production of neoantigens during SARS-CoV-2 infection.
These neoantigens arise when the virus's two proteases—NSP3 (papain-like protease, PLPro, sometimes referred to as MPro in the paper) and NSP5 (3C-like protease, 3CLPro)—cleave not only viral proteins but also thousands of human host proteins in infected cells.
This cleavage generates novel peptide fragments (neoantigens) that the immune system misrecognizes as foreign, leading to autoreactive T-cell responses, production of functional autoantibodies (fAABs), chronic inflammation, and diverse autoimmune symptoms.
The author estimates this mechanism affects ~10% of all SARS-CoV-2-infected individuals worldwide, explaining the wide variability in LC symptoms (from organ-specific damage to systemic conditions like myalgic encephalomyelitis/chronic fatigue syndrome, ME/CFS).
Key Evidence and Data
Bioinformatics analysis of the human proteome (~72,000 proteins) shows SARS-CoV-2 proteases target approximately 6,500 human proteins (NSP3: ~602; NSP5: ~6,439; some overlap). This is based on consensus cleavage sites ("L-GG•A/K" and "LQ•A/S").
In contrast, common latent viruses target far fewer human proteins (e.g., EBV: 2; HSV6/7: 3; other Herpesviridae: 8–50; CMV: 68), making neoantigen-driven autoimmunity less likely in those infections (where molecular mimicry via "mimotopes" plays a larger role).
Other viruses/parasites (e.g., rhinoviruses: ~11,577 targets; flaviviruses/hepaciviruses: 7,198–20,516) cleave more but are adapted for persistence without overwhelming immune attack.
Post-infection studies (e.g., in hamsters and humans) show ~90% of antibodies target host proteins rather than viral ones.
Cleavage disrupts key pathways (e.g., IL-12/IL-35 signaling via JAK1/2, TYK2, STAT1/4), impairing interferon responses and viral clearance, contributing to persistence.
Proposed Mechanisms and Symptoms
Neoantigens are presented on MHC molecules → chronic CD8+/CD4+ T-cell activation → fAABs (especially against G-protein-coupled receptors, GPCRs) → symptoms like vascular damage, multi-organ failure, thrombosis, neurocognitive issues, hypertension, type II diabetes, dementia, and chronic fatigue.
Additional factors: Complement dysregulation, CD8+ T-cell loss, EBV reactivation, and interferon inhibition by viral proteins.
Conclusions and Implications
The pandemic is "not yet over" due to ongoing Omicron evolution (~4 new strains/year).
Prevention: Annual targeted vaccinations (mRNA or classical) reduce LC risk by ~45–50%; repeated infections increase it.
Treatment ideas: Protease inhibitors (e.g., Paxlovid targeting NSP5), aptamers like BC007 (to neutralize fAABs against GPCRs, in trials), or apheresis.
The hypothesis explains LC's heterogeneity and diagnostic challenges, as outcomes depend on individual MHC presentation of neoantigens.
This is a theoretical/commentary piece based on bioinformatics and existing literature, not new experimental data. The full open-access article is available online (e.g., via Scientific Archives or ResearchGate). Other reviews discuss related ideas like molecular mimicry or autoimmunity in Long COVID, but Marschalek's focus is uniquely on protease-generated neoantigens as the dominant driver.
----
>>>>so what is the difference between protease-generated neoantigens and autoimmunity and mimicry?
Molecular Mimicry vs. Protease-Generated Neoantigens in Autoimmunity
Autoimmunity occurs when the immune system mistakenly attacks the body's own tissues. Both molecular mimicry and protease-generated neoantigens are proposed mechanisms that can trigger autoimmunity during or after viral infections, but they operate in fundamentally different ways.
1. Molecular Mimicry
This is the classic, long-established mechanism.
Viral proteins (or peptides derived from them) happen to share sequence or structural similarity with human host proteins.
The immune system generates antibodies or T-cells against the viral peptides.
These immune effectors cross-react with similar-looking human proteins because of the resemblance (called "mimotopes").
Result: Autoimmunity without any direct modification of host proteins.
Common in infections with latent viruses like Epstein-Barr Virus (EBV), Herpesviruses, or CMV, where only a handful of human proteins are subtly similar to viral ones.
The similarity is coincidental or evolutionary, and the host proteins remain intact and unchanged.
2. Protease-Generated Neoantigens (as proposed by Marschalek for SARS-CoV-2)
This is a more direct and aggressive mechanism unique to viruses with highly active proteases.
SARS-CoV-2 has two viral proteases (NSP3/PLpro and NSP5/3CLpro) that cleave viral polyproteins but also extensively cleave thousands of human host proteins at specific consensus sites.
This cleavage physically breaks human proteins into novel peptide fragments that did not exist before in the body.
These brand-new fragments ("neoantigens") are presented on MHC molecules to T-cells.
The immune system treats them as completely foreign (because they are truly novel sequences), mounting a strong response against them.
Since these neoantigens are derived from self-proteins, the response becomes autoreactive → autoantibodies and T-cell attack on intact host proteins or cells expressing them.
No sequence similarity to viral proteins is required—the damage is done by literally chopping up host proteins.
In Marschalek's hypothesis, SARS-CoV-2's unprecedented protease activity on host proteins makes neoantigen-driven autoimmunity the dominant mechanism for Long COVID, rather than mimicry (which plays a bigger role in other viral-triggered autoimmune diseases).
This explains why Long COVID affects ~10% of infections with such diverse symptoms—individual MHC presentation of different cleaved peptides leads to personalized autoimmune profiles. Mimicry alone couldn't generate enough "new" targets to account for the observed breadth.